Locations:
Tongue-tie is a condition that limits the function of your baby’s tongue. Some babies have difficulty latching on for breastfeeding or taking in enough milk. Often, support from a lactation consultant can help you adjust your position and latch for successful breastfeeding. Some babies with tongue-tie need a procedure to help their tongues move better.
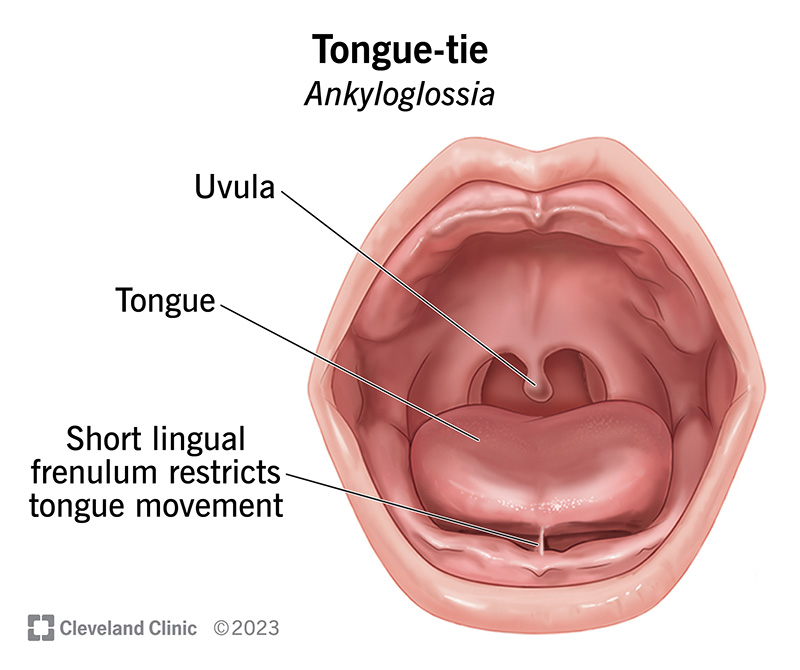
Tongue-tie is when a baby’s tongue can’t move as well as it should because a fold of tissue connects the bottom of their tongue to the floor of their mouth. This fold of tissue, called the lingual frenulum, is present in all children and usually harmless. But sometimes, a lingual frenulum that’s too tight or short can restrict the movement and function of a baby’s tongue. When this happens, healthcare providers diagnose a baby with ankyloglossia, more commonly known as tongue-tie.
Tongue-tie can sometimes pose challenges for breastfeeding (chestfeeding). Babies with tongue-tie may have trouble latching on or removing milk. This can prevent them from getting enough nutrition. Latching difficulties can also cause pain or discomfort for the breastfeeding parent, who may feel they need to stop breastfeeding.
If this sounds familiar, don’t give up. Often, lactation consultants can help you adjust your breastfeeding position or your baby’s latch to overcome these challenges. If these methods aren’t enough, your baby may need a safe and quick procedure called a frenotomy. This involves clipping the lingual frenulum so your baby’s tongue can move freely.
Your lactation consultant and pediatrician will work with you to find the best solution so both you and your baby can feel better.
Anywhere from 1% to 11% of newborns have signs of ankyloglossia, according to the American Academy of Pediatrics. The condition appears to be more common in babies assigned male at birth (AMAB).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Ankyloglossia symptoms in newborns include:
If you’re breastfeeding, you may also have symptoms related to your baby’s tongue-tie, including:
Keep in mind that these symptoms are what healthcare providers call nonspecific. That means they’re not unique to tongue-tie, specifically, and could occur for many other reasons. That’s why it’s important to see a healthcare provider with experience in managing breastfeeding issues. They’ll help identify the cause of your symptoms (whether it’s tongue-tie or something else) and find a solution.
Your baby’s tongue may appear to be heart-shaped or may have a notch in it. That’s because the lingual frenulum connects near the tip of their tongue and restricts its movement. In some cases, tongue-tie is barely noticeable. Healthcare providers look for signs of tongue-tie during a physical exam soon after birth.
Tongue-tie is congenital, which means your baby is born with it. Researchers aren’t exactly sure why some babies are born with tongue-tie, but there may be a genetic component. Some research suggests tongue-tie may be passed down within families, possibly in an X-linked pattern of inheritance.
Advertisement
Pediatricians typically diagnose tongue-tie soon after a baby is born. They work with lactation consultants, who can identify whether variations in a baby’s tongue anatomy may cause breastfeeding difficulties.
Just because a baby has a frenulum that’s tighter or shorter than usual doesn’t mean they have tongue-tie or need treatment. Healthcare providers only diagnose this condition in babies who have a restrictive lingual frenulum and limited tongue function.
To determine if your baby has tongue-tie, your providers will:
Your baby doesn’t need any tests. Some healthcare providers use different grading systems or assessment tools that evaluate how well a baby’s tongue moves in their mouth. But they get the information they need just by looking at your baby’s tongue and feeling the lingual frenulum.
These grading systems help providers describe how a baby’s tongue looks and functions. This information can help providers reach a diagnosis.
Healthcare providers manage tongue-tie by:
Many babies with tongue-tie don’t need surgery. And if your baby does need treatment, you can rest assured it’s not major surgery. In fact, healthcare providers can often clip a baby’s lingual frenulum in a quick in-office procedure called a frenotomy.
Often, babies with tongue-tie don’t need this procedure at all. Providers only suggest a frenotomy if changes to your breastfeeding position and your baby’s latch don’t resolve the symptoms.
This safe procedure is the gold standard for treating infants with tongue-tie. Before doing a frenotomy, healthcare providers rule out or treat other causes of breastfeeding difficulty. When a frenotomy is necessary, it’s typically best when done within the first month of a baby’s life. This allows your baby to establish effective breastfeeding habits early on.
A frenotomy is generally a safe procedure and has a low risk of complications. Rarely, babies experience:
Advertisement
There’s no known way to prevent tongue-tie. For more severe cases, early diagnosis and treatment can prevent issues with breastfeeding.
Tongue-tie isn’t usually a cause for worry. It’s common and often manageable without doing a procedure. The key is seeking help early. Don’t wait or think the situation will get better if you just try harder. Breastfeeding difficulties aren’t your fault, and they’re very common. Even experienced parents sometimes need expert advice to solve issues that come up.
Tongue-tie rarely poses problems with bottle feeding. Your baby’s tongue works differently when feeding from a bottle compared with feeding from a breast. If needed, a lactation consultant can modify the bottle’s nipple or flow to help with any issues that arise. If your baby continues struggling with bottle feeding, there may be other factors at work. Your lactation consultant and pediatrician will work together to find the cause.
If your baby has trouble with nursing, reach out to a healthcare provider. Whether or not tongue-tie is the cause, a lactation consultant can work with your pediatrician to give you the support you need.
There’s currently no evidence that tongue-tie causes sleep apnea in children, according to a clinical consensus statement published in 2020.
Experts agree that tongue-tie usually doesn’t affect a child’s speech. So, there’s no need for a baby to have a frenotomy in an attempt to prevent future speech disorders.
The term posterior tongue-tie refers to a portion of the lingual frenulum that extends more into the substance of a baby’s tongue in the floor of the mouth, as opposed to closer to the tip. However, this is a controversial term. Some healthcare providers have suggested it’s anatomically inaccurate and recommend getting rid of it. They prefer just using the term tongue-tie regardless of the exact location of the lingual frenulum.
A lip tie typically refers to the band of tissue that connects your baby’s upper gum with their upper lip. This band of tissue, called the maxillary labial frenulum, has many normal variations. Just because it connects farther down on your baby’s gumline or seems more prominent doesn’t mean it’s going to cause problems.
Still, lip tie is a controversial topic among healthcare providers. Some believe that a lip tie can cause breastfeeding issues or later dental issues. Others believe there’s not enough evidence to prove these connections.
When it comes to breastfeeding, the latest research shows procedures to treat lip tie aren’t necessary. There’s simply not enough evidence to show that releasing a lip tie improves milk transfer or eases nipple pain. However, if you’re concerned about your baby’s latch, talk to a lactation consultant.
Tongue-tie can affect some adults, but it’s usually diagnosed and treated in babies. The lingual frenulum (below the tongue) is just one example of a fold or band of tissue inside your mouth. Other tissues, like the buccal (cheek) frenula, provide support in other areas of your mouth. Depending on their size or location, they can make it hard to clean your teeth or gums fully. Your dentist can evaluate all the structures inside your mouth and let you know if there are any concerns.
A note from Cleveland Clinic
The first month of your baby’s life is full of wonder and discovery for you both. But it can also bring exhaustion and frustration, especially if breastfeeding isn’t going as planned. Tongue-tie is one possible cause of breastfeeding difficulties. But it’s definitely not the only one. If your baby has trouble with feedings, don’t hesitate to reach out to a lactation consultant. They’ll work with your pediatrician to find the cause and tailor a solution to your needs.
Last reviewed on 02/06/2024.
Learn more about the Health Library and our editorial process.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy