Locations:
Ulcerative colitis (UC) is a chronic condition that happens when you have inflammation in your colon. Most people with UC experience periods of symptom flare-ups followed by periods of remission without symptoms. Signs and symptoms include diarrhea, bloody stools, abdominal cramping and weight loss Treatments include medication and surgery.
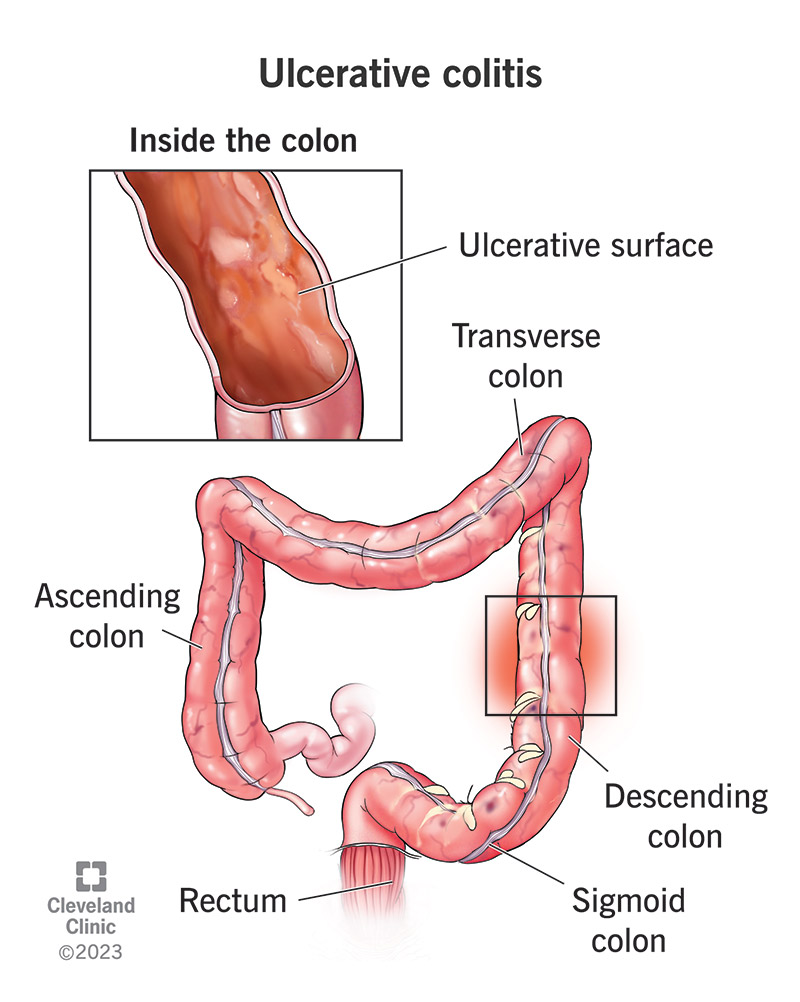
Ulcerative colitis (UC) is a lifelong condition that causes inflammation and ulcers inside your colon (large intestine). UC is one of the most common types of inflammatory bowel disease (IBD), alongside Crohn’s disease. UC often causes bloody diarrhea and abdominal cramping. It may make you have to poop more.
Most people with UC experience periods when they experience symptoms (flare-ups), followed by longer periods of no symptoms (remission).
Healthcare providers classify UC based on where the inflammation is in your colon. The inflammation usually starts in your rectum, which is close to your anus (butthole). The inflammation can spread and affect all or part of your colon. Types include:
UC may be mild, moderate or severe, depending on your symptoms. The most severe form, fulminant ulcerative colitis, is rare. It can cause life-threatening complications that require urgent medical treatment.
Together with Crohn’s disease, another type of inflammatory bowel disease, UC affects up to 1 in 250 people in North America and Europe. According to the National Institute of Diabetes and Digestive and Kidney Diseases (U.S.), up to 900,000 people in the U.S. are living with UC.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Ulcerative colitis symptoms often get worse over time. In the beginning, you may notice signs of mild UC, including:
Later, you may also have symptoms of moderate to severe UC, including:
About half of people have mild symptoms during flare-ups. Others experience frequent fevers, bloody diarrhea, nausea and severe abdominal cramps.
About 25% of people with UC eventually develop conditions and associated symptoms that affect body parts other than their colon. The inflammation can spread to your bones, joints, eyes, skin and liver.
Symptoms include:
Researchers think the cause of ulcerative colitis is complex and involves many risk factors. Most agree that it’s related to an overactive immune response. Your immune system’s job is to protect your body from germs and other dangerous substances. But sometimes, your immune system mistakenly attacks your body, which causes inflammation and tissue damage.
Anyone can get ulcerative colitis, but your risk is greater based on your:
Other factors, like stress and your diet, don’t increase your risk of developing UC, but they can trigger a symptom flare-up. One of the best things you can do if you’re diagnosed with UC is to note your triggers so you can avoid them.
Advertisement
Having ulcerative colitis raises your risk of developing other conditions that may require additional monitoring and treatment, including:
Emergency complications of UC that require immediate treatment in the ER include:
To diagnose UC, your healthcare provider will perform a physical exam and ask about your symptoms and family history of IBD. They’ll order tests and perform procedures to rule out conditions similar to UC.
Tests and procedures include:
Advertisement
The goal of treatment is to put you into remission if you’re experiencing a flare-up or help you maintain remission if you’re not currently experiencing symptoms. Treatment options include medications and surgery.
Healthcare providers use several medications (alone or in combination) to calm inflammation in your large intestine. Reducing the swelling and irritation lets the tissue heal. It can also relieve your symptoms so you have less pain and diarrhea.
Medications for UC include:
Surgery is an option if medications aren’t working or if you’re experiencing serious complications. About 30% of people with ulcerative colitis need surgery at some point. About 20% of children with ulcerative colitis will need surgery.
There are two kinds of surgery for ulcerative colitis. Both involve a proctocolectomy, surgery to remove all or part of your colon and rectum.
You can reduce your likelihood of a flare-up by identifying and avoiding your triggers. Tips for avoiding common triggers include:
It’s a good idea to note your triggers in a diary you can share with your provider. Together, you can work on strategies to avoid things that may cause a flare-up.
A few people have one flare-up and never have another. Others have chronic symptoms that are difficult to manage. Most people have symptoms that come and go, with periods of flare-ups and longer periods of remission. In up to 30% of people, ulcerative symptoms worsen and happen more often. Eventually, they’ll need surgery.
Most people manage UC by avoiding triggers and taking medicines regularly to prevent inflammation. You’ll also need frequent provider visits to monitor your health. For example, depending on your risk, you may need regular colonoscopies to screen for colon cancer. Your provider can advise you.
The only “cure” for UC is surgery to remove your colon and rectum. Still, most people can manage UC with medications or surgery. With UC treatment, the goal is achieving and maintaining remission. Your healthcare provider can help you get there.
Call your healthcare provider immediately if you have:
Questions to ask include:
A note from Cleveland Clinic
It’s essential to work closely with your healthcare team if you have ulcerative colitis. Take your medicines as prescribed, even when you don’t have symptoms. Skipping your medicine can lead to flare-ups and make your condition harder to manage. Make sure you understand how your risk of complications impacts your care. For example, you may need more frequent blood tests or colonoscopies than someone without UC. Ask how your care plan will increase your likelihood of staying in remission while promoting your overall health.
Last reviewed on 11/05/2023.
Learn more about the Health Library and our editorial process.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy